

Background: The past two decades have seen an explosion in the development of new drugs for the treatment of myeloma, and previous studies have shown that these advances have translated into improved survival. It is unclear if we have continued to maintain the pace of improvement in the recent years. We designed this study to examine the patterns of survival in patients with newly diagnosed MM, specifically examining the impact on patient subgroups by age and disease risk.
Patients and Methods: We included patients with newly diagnosed MM, who were seen at Mayo Clinic, Rochester between 2004 and 2018. We grouped them into three 5-year groups: group 1 (2004-2008), group 2 (2009-2013) and group 3 (2014-2018) to assess the trends over time. Only those who were seen within 6 months of diagnosis were included in the current cohort. Fluorescence in situ hybridization (FISH) was performed using clg based approach as previously described and high risk (HR) was defined as those with t(4;14), t(14;16), t(14;20) and del17p. Survival was estimated using the Kaplan-Meier method and curves were compared using the log rank test. The Cox proportional hazards model was used to examine the prognostic impact of various clinical and laboratory factors.
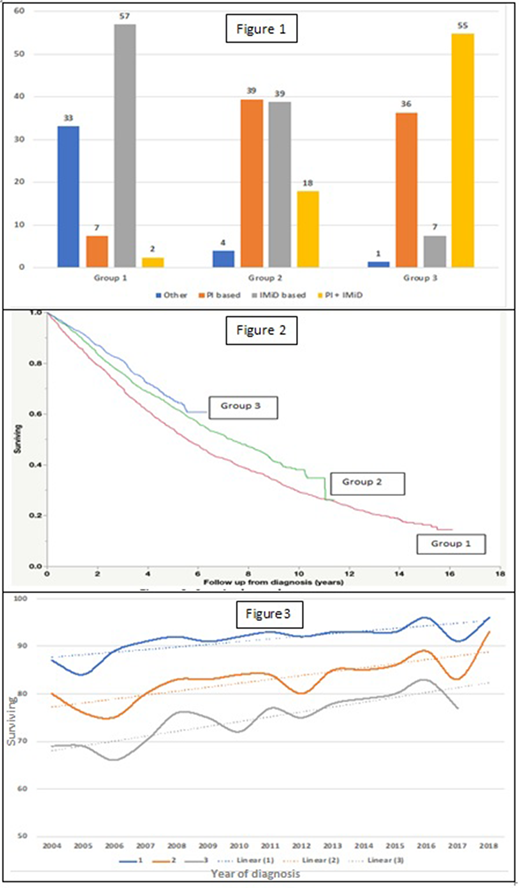
Results: The study cohort had 3783 patients: 61% were male, median age was 64 years (range 22-96), 47% were ≥65 and 14% ≥75 years. There was no change over time in the median age or the gender distribution. No clear trends were evident across the groups in terms of the disease characteristics including high risk status. The patients in the cohort were divided into three 5 year groups: Group 1(2004-2008; n=1045), Group 2(2009-2013; n=1237) and Group 3(2014-2018; n=1501). The initial treatment regimen changed over time to include proteasome inhibitors (PI) and immunomodulatory drug (IMiD) based regimens with a PI-IMiD combination being 2%, 18% and 55% respectively in groups 1, 2 and 3 (Figure 1). The median follow-up for the entire cohort was 6.8 years (95% CI; 6.5,6.9), and for groups 1, 2 and 3 were 13 years, 8 years and 3.2 years respectively. The median OS for the entire group was 6.8 years (95% CI; 6.4, 7.2). The median OS from diagnosis has improved over time with the groups 1, 2, and 3 having a median OS (95% CI) of 5.5 years (5.1, 6.1), 7.3 years (6.7, 8.0) and NR respectively(P=0.0001) (Figure 2). We specifically looked at the 1, 2 and 3-year survival over the years and found a steady trend for improvement (Figure 3). When examining trends by age, those under 65 years had improvement in survival from group 1 to 2; median OS was 7.3 years, 10 years and NR for groups 1, 2 and 3 respectively (P=0.0001) . Those above 65 had major improvement from group 2 to 3; median OS was 4.4 years, 5.2 years and NR for groups 1,2 and 3 respectively (P=0.0001). When examined by FISH risk status, improvement in OS was seen among with Standard Risk (SR) status, especially during the last 5-year period. The median OS for patients with HR status was 3.5 years, 4.5 years and NR (P=0.07); and 7.6 years, 8.6 years and NR in patients with SR status (P=0.0012) for groups 1, 2 and 3 respectively.
Conclusion: In a large cohort of patients with newly diagnosed MM, we have been able to demonstrate sustained improvement in OS over the years, likely driven by introduction of new drugs and continued use of transplant. The impact of newer generation of drugs, especially monoclonal antibodies is not reflected in this analysis and will likely become obvious over the next five years. The data will help identify the areas that require focus for continued improvements in order to derive the maximum impact on outcomes.
Kapoor:Celgene: Honoraria; Amgen: Research Funding; Sanofi: Consultancy, Research Funding; Janssen: Research Funding; Cellectar: Consultancy; GlaxoSmithKline: Research Funding; Takeda: Honoraria, Research Funding. Gertz:Alnylam: Other: personal fee; Prothena: Other: personal fee; Teva: Speakers Bureau; Johnson and Johnson: Speakers Bureau; DAVA oncology: Speakers Bureau; Proclara: Other; Aurora Bio: Other; Springer Publishing: Patents & Royalties; Sanofi: Other; Research to Practice: Other; Celgene: Other; Physicians Education Resource: Other: personal fee; Medscape: Other: personal fee, Speakers Bureau; Amgen: Other: personal fee; Appellis: Other: personal fee; Annexon: Other: personal fee; Spectrum: Other: personal fee, Research Funding; Janssen: Other: personal fee; Ionis/Akcea: Other: personal fee; Abbvie: Other. Dispenzieri:Intellia: Research Funding; Alnylam: Research Funding; Takeda: Research Funding; Pfizer: Research Funding; Janssen: Research Funding; Celgene: Research Funding. Dingli:Rigel: Consultancy; Bristol Myers Squibb: Research Funding; Apellis: Consultancy; Alexion: Consultancy; Sanofi-Genzyme: Consultancy; Karyopharm Therapeutics: Research Funding; Millenium: Consultancy; Janssen: Consultancy. Russell:Imanis: Other: Equity Ownership. Lin:Juno: Consultancy; Bluebird Bio: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Novartis: Consultancy; Takeda: Research Funding; Legend BioTech: Consultancy; Merck: Research Funding; Vineti: Consultancy; Janssen: Consultancy, Research Funding; Kite, a Gilead Company: Consultancy, Research Funding; Sorrento: Consultancy, Membership on an entity's Board of Directors or advisory committees; Gamida Cells: Consultancy. Kumar:Carsgen: Other, Research Funding; Adaptive Biotechnologies: Consultancy; Tenebio: Other, Research Funding; Celgene/BMS: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Cellectar: Other; Genecentrix: Consultancy; Dr. Reddy's Laboratories: Honoraria; Janssen Oncology: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Novartis: Research Funding; Kite Pharma: Consultancy, Research Funding; Takeda: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; MedImmune: Research Funding; Sanofi: Research Funding; Karyopharm: Consultancy; Oncopeptides: Consultancy, Other: Independent Review Committee; IRC member; BMS: Consultancy, Research Funding; Genentech/Roche: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Merck: Consultancy, Research Funding; Amgen: Consultancy, Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments, Research Funding; AbbVie: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments.

